The Physiology of Chokes in BJJ: Science, Technique and Safety
By Javier Feliubadaló
Introduction
In Brazilian Jiu-Jitsu (BJJ) and mixed martial arts (MMA), chokes are highly effective and widely used submission techniques. At Circle Academy Barcelona, where we train gi and no-gi BJJ as well as mixed martial arts, we believe technique must be backed by knowledge. This article takes a deep dive into the physiology of blood chokes: how they work, why they are so effective, what sets them apart from other forms of asphyxiation, and what precautions should be taken to ensure safe practice.
What Is a Blood Choke?
A blood choke, or carotid strangle, cuts off the supply of oxygenated blood to the brain by compressing the internal carotid arteries on both sides of the neck. This interruption causes loss of consciousness within seconds. Techniques such as the rear naked choke (mata leão), the triangle choke, and lapel chokes (like the cross-collar choke with the gi) are classic examples.
Unlike air chokes (which block airflow through the trachea or prevent inhalation), blood chokes act directly on cerebral circulation, allowing the practitioner to subdue an opponent more quickly, in a more controlled manner, and more safely when executed correctly.
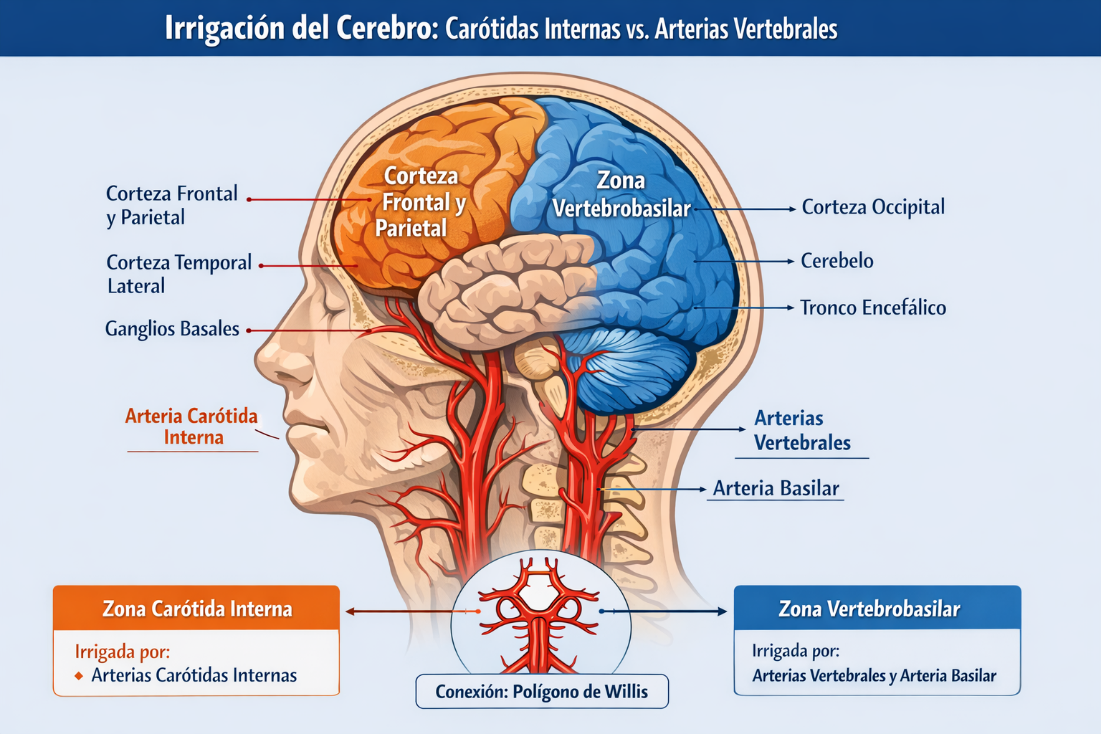
Cerebral Vascular Supply: Internal Carotids vs. Vertebral Arteries
The brain receives blood from two main arterial systems:
Anterior Carotid System
- Main vessel: Internal carotid artery (ICA)
- Supplies: The anterior two-thirds of the brain
Vertebrobasilar System (Posterior)
- Main vessels: Vertebral arteries, which join to form the basilar artery
- Supplies: The posterior third of the brain (brainstem, cerebellum, and occipital lobe)
Connection: The Circle of Willis
Both systems communicate at the base of the brain through the Circle of Willis, which allows a degree of cross-compensation when one artery is obstructed. For example, if the right vertebral artery fails, blood flow can be redistributed from the left side or from the internal carotid via the anterior and posterior communicating arteries.
Relevance to the Blood Choke (BJJ)
When a choke effectively compresses the internal carotid arteries, it cuts off blood supply to the majority of the cerebral hemispheres (frontal cortex, parietal cortex, and part of the temporal cortex), causing rapid unconsciousness.
The vertebrobasilar system (vertebral and basilar arteries), which supplies the brainstem and cerebellum, may maintain some blood flow when the carotids are compressed, but this is not enough to sustain consciousness — the cerebral cortex demands the most oxygen.
The Role of the Carotid Sinus and the Vagal Reflex
A key factor in the effectiveness of blood chokes is the stimulation of the baroreceptors in the carotid sinus, located at the bifurcation of the common carotid artery (C4 level). Applying pressure to this area activates a vagal reflex that can trigger a sudden drop in blood pressure and heart rate, causing a carotid sinus syncope — even if the arterial occlusion is not complete.
The vertebral arteries run through the transverse foramina of the cervical vertebrae (C6 to C1), protected by bony structures. This makes them far less susceptible to direct external compression during a choke like the rear naked choke.
In contrast, the internal carotid arteries are more superficial and accessible on the sides of the neck, making them the primary physiological target of a blood choke.
The rear naked choke does not directly compress the vertebral arteries. Its primary action is on the internal carotid arteries (and sometimes the jugular veins), which are more accessible to external pressure. Vertebrobasilar compression could only be affected indirectly, if at all, by extreme displacement or cervical injury — but not as the normal mechanism of a blood choke.
In IBJJF and AJP rulesets, spinal attacks without a choke are prohibited, as is any cervical traction on children.
The Baroreceptor Hypothesis
The remarkable efficacy of blood chokes is largely based on baroreceptors — compressing just one side of the neck can also produce a blackout. This hypothesis is supported by real physiological evidence: the baroreceptors of the carotid sinus, when stimulated by pressure, can trigger an intense vagal reflex response (bradycardia, peripheral vasodilation, and a drop in blood pressure) leading to carotid sinus syncope.
This would explain why:
- Unilateral chokes (such as an off-center Guillotine or rear naked choke, D'Arce, Anaconda, Peruvian Choke, Von Flue, Canto Choke, Kata Gatame, etc.) can also cause loss of consciousness, even without complete bilateral blood flow occlusion.
- The pressure does not even need to fully block the carotid lumen — mechanically stimulating the carotid sinus is enough for the brain to respond by lowering cerebral perfusion.
- In people with carotid sinus hypersensitivity, a light touch or brief pressure on one side of the neck can induce immediate fainting — a well-documented medical phenomenon.
It is likely that much of the "blackout" in a rapid choke is not solely due to ischemia, but also to the vagal reflex induced by pressure on the carotid sinus. This explains the surprising speed of some BJJ knockouts even with seemingly partial or "loose" technique.
Cerebral Tolerance Time Without Oxygen
It is crucial to understand how long the human brain can tolerate a lack of oxygen before suffering permanent neurological damage. Scientific evidence establishes the following margins:
| Time | Effect |
|---|---|
| 0–10 seconds | Reversible loss of consciousness (syncope) |
| 30–60 seconds | Possible onset of myoclonus or transient spasms |
| 2–3 minutes | Recovery still possible without permanent damage if circulation is restored |
| 3–5 minutes | Increased risk of irreversible brain damage |
| >5 minutes | High probability of permanent injury or brain death |
In the context of BJJ, an effective choke causes unconsciousness in under 10 seconds and, if released immediately, carries no neurological consequences. These figures are supported by studies such as Hossmann (Critical Care Medicine), Safar & Bircher (Textbook of Critical Care), and Neumar et al. (Circulation).
Anatomy: Which Arteries Are Involved?
The internal carotid arteries are primarily responsible for blood supply to the anterior cerebral hemispheres (frontal, parietal, and lateral temporal lobes). They are superficial and therefore accessible to compression during a choke.
The vertebral arteries, on the other hand, pass through the transverse foramina of the cervical vertebrae and merge to form the basilar artery. They supply the brainstem, cerebellum, and occipital lobe, but are far more protected by bony structures. It is very unlikely they would be compressed during a technique like the rear naked choke.
Additional Consideration: Cervical Rotation and Vertebral Arteries
Studies have shown that cervical rotation can reduce or even interrupt flow through one of the vertebral arteries, which has both clinical and sporting implications.
- The vertebral arteries ascend through the transverse foramina of the cervical vertebrae and enter the skull through the foramen magnum.
- At C1-C2, they curve (atlantoaxial portion), making them more vulnerable to stretching and compression during head rotation.
- In healthy individuals, one vertebral artery may partially close when the head is turned, but flow is compensated by the contralateral artery through the basilar system.
- In individuals with unilateral vertebral hypoplasia, stenosis, or malformations, this closure can cause symptoms: dizziness, blurred vision, syncope, or even brainstem stroke — known as vertebral artery syndrome.
In positions such as:
- Guillotines with forced neck rotation
- Defending the rear naked choke by forcing the chin laterally
- Neck cranks or explosive movements with cervical torsion
It is theoretically possible that the combination of external pressure and rotation could affect vertebrobasilar flow in certain individuals. This could contribute to the "blackout" in cases where the technique does not appear to be fully locked in.
Comparison: Blood Choke vs. Air Choke vs. Smothering
| Type | Mechanism | Speed | Risk |
|---|---|---|---|
| Blood choke | Compression of carotid arteries | 5–10 seconds | Low (if released in time) |
| Air choke | Tracheal / airway blockage | 30–60+ seconds | Higher (soft tissue damage) |
| Smothering | Obstruction of mouth/nose or chest compression | Variable | Variable (depends on control) |
Smother Chokes: A Special Case
In some situations, especially in no-gi grappling or self-defense, an opponent may be immobilized and unable to breathe due to pressure over their face blocking the mouth and nose, or through thoracic compression. This type of asphyxiation — known as mechanical smothering — does not act on the neck or the internal airways but prevents external ventilation.
Examples:
- Chest pressure from high mount over the opponent's face.
- Covering the mouth and nose with the hand (sometimes called a "mother choke" or "smother choke").
- Chokes combined with thoracic compression, such as body triangles or aggressive knee-on-belly.
These techniques were not traditionally taught as formal finishes, but they can induce a tap through claustrophobia, panic, or respiratory fatigue. In sport BJJ they were sometimes frowned upon or regulated, but they are increasingly used and are perfectly valid in self-defense.
Safety and Risks
Although properly applied blood chokes are safe and reversible, risks exist if they are maintained beyond the point of unconsciousness or applied with excessive force:
- Arterial injury (dissection): extremely rare, but possible with sudden cervical movements.
- Carotid sinus hypersensitivity: may induce sudden reflex syncope.
- Tracheal or soft tissue injuries: more common with air chokes.
- Prolonged smothering without control: can be dangerous if not detected in time.
- Brief seizures or myoclonus: occasional after blackouts, generally benign.
At Circle Academy, we emphasize clean technique, respect for the tap, and progressive control to prevent these complications.
Conclusion
Chokes are powerful and effective tools within the technical arsenal of BJJ and grappling in general. Their effect is based on the interruption of cerebral blood flow, reflex mechanisms such as carotid sinus stimulation, and the impediment of airflow. Understanding these processes not only improves technique but also allows for safer and more conscious training.
At Circle Academy (Barcelona) we foster a technical, scientific, and respectful approach to martial arts practice. If you train or teach BJJ, it is vital that you understand not only how to apply a choke, but the science behind it and why it works.
Interested in learning more about BJJ, MMA, or Submission Grappling with a technical and mindful approach? Visit us at Circle Academy and train with us in the heart of Barcelona.
References
- Hossmann KA. (1971). "Cerebral ischemia: tolerance and thresholds." Critical Care Medicine.
- Safar P, Bircher N. (1988). Textbook of Critical Care.
- Neumar RW et al. (2008). "Post–cardiac arrest syndrome." Circulation.
- De La Sayette V et al. (1991). "Syncope and cerebral hypoperfusion." Neurology.
- Sterz F et al. (1985). "Recovery from prolonged cerebral ischemia in dogs." Stroke.
- Bujinkan Asturias (2017). Shime Waza. Types of strangulation: air choke vs. blood choke.
- Fernando Cadena BJJ (2016). Chokes in Jiu-Jitsu. Carotid sinus and baroreceptor reflex.
- Kenhub (2023). Internal Carotid Artery – Anatomy.
- Revista Artes Marciales Asiáticas (2009, Vol 4 No.1). "The carotid strangle: to sleep, perchance to die?" (Wedlake & Rowe).
- FightingArts (Neil Ohlenkamp). The Judo Choke.
- Radical MMA NYC (R. Marinoble, 2016). "Anatomy of the Air Choke."
- Jiu-Jitsu Medicine (A. Walls, MD, 2023). "Choke Physiology."
- Harrington et al. (2024). "Exploring Choke Holds in BJJ Athletes." Orthopedic Journal of Sports Medicine.